By: Robert Francis Sidonio, Jr., MD, MSc.
Published: Lifelines for Health Summer 2020
Women and Girls Clinics
The recognition of the unique challenges of women with bleeding disorders has quickly expanded over the last 2 decades. In 1998, a seminal article was published by Dr. Peter Kouides highlighting the “silent majority” and setting the stage for the hard work needed to meet these challenges. Back then we knew that it would take a wider medical community to address the needs of women with bleeding disorders (WWBD).
The focus has been to increase awareness amongst healthcare providers focusing first with the hematologists and then other medical providers that are an essential part of a woman’s healthcare including adolescent medicine, gynecology oncology, and primary care providers. Additionally, because of large gaps in care, a multidisciplinary approach would be required. It made sense that the same approach used successfully for men with bleeding disorders, specifically males with hemophilia, would be ideal for WWBD. Modifications of this model were needed of course. This multidisciplinary team that was in place for decades as part of the hemophilia treatment center (HTC) model and established a solid foundation for the creation of the first “women and girls clinics.” Typically, the clinic model employed a hematologist, nurse and gynecologist or adolescent medicine provider. As with the multidisciplinary HTC model, social workers, genetic counselors, and physical therapists are added as available and needed. Most of these women’s clinics are conducted on a recurrent basis, typically once or twice a month. The approach may vary slightly based on hospital or clinic infrastructure. The patient may be seen separately by the hematologist and gynecologist/adolescent medicine provider or together, my preferred strategy. To make this model work from a financial perspective, the gynecologist or adolescent provider may have a portion of their salary covered utilizing 340B funding, a program created by Congress allowing the HTC to purchase clotting factor concentrates (CFCs) at a discount price with the savings going directly into providing services for the patient, including paying for the salaries of the HTC staff and clinical research initiatives.
Thankfully, more patients are being identified and managed with expertise improving. This is seen in the number of patients registered in various surveillance programs such as the CDC Community Counts and ATHNdataset. All of these collect basic demographic data and limited information on bleeding events and diagnostic labs and in some cases limited information on quality of life, or the affect the bleeding disorder has on the person’s life. There are some targeted initiatives that have been ended such as Female Universal Data Collection which summarized data on >300 WWBD from 17 HTCs from 2009-2011. Similarly, the My Life our Future Project had a pilot allowing collection of clinical bleeding symptoms and genetic testing in >1000 hemophilia A and B carriers. Ongoing research projects will be discussed later in this article. As a result of more focus on WWBD, the number of women and girls clinics has grown from a handful in the early 2000s to >150 in 2020. These clinics offer a variety of services for WWBD and best practices are currently shared at yearly Learning Action Network meetings sponsored by the Foundation for Women and Girls with Blood Disorders.
Following a few articles in the early to mid 1990s highlighting our lack of ability to address the needs of WWBD, from 1990-2010 there was an exponential rise in the number seen at HTCs at a much higher rate than their male counterparts. It is reassuring that to see the general trend of WWBD being managed by the same top-notch hemophilia providers as their male counterparts. But are their clinical and research needs
being met?
Despite all of the aforementioned progress, there is certainly a gap in the recognition that WWBD may have significant bleeding and a lack of standard practice in the management over their lifetime. The solution to this lies in an improved focus on clinical research in WWBD which over time will translate into improved care and recognition from some reluctant colleagues and payors.
Advocacy Organizations
The Foundation for Women and Girls with Blood Disorders (FWGBD) was launched in 2010 as a non-profit organization with a focus on provider education across all disciplines to ensure women and girls with blood disorders are diagnosed and appropriately managed over their lifetime. This organization has a robust group of mentored young physicians interested in clinical research and innovation in practice and has led to multiple research initiatives. Although the initial focus was on women and girls with bleeding and clotting disorders, blood disorders such as sickle cell disease, thalassemia, and immune thrombocytopenia are being addressed more over the last 3 years.
While FWGBD focuses on provider education and developing a medical community of dedicated researchers and master clinicians, patient advocacy organizations such as the National Hemophilia Foundation (NHF) and Hemophilia Federation of America (HFA) have dedicated programs to women and girls with bleeding disorders. Victory for Women (victoryforwomen.org) is an NHF initiative created to provide support, education, and resources for women and providers in the bleeding disorders community. The main goal is to address critical issues and ultimately improve quality of life for women in this tightknit community. It recently was rebooted with additional support. HFA has created a Women Bleed Too! Toolkit (hemophiliafed.
org) organizing their resources amassed over the years into one location. Acknowledging poor communication between providers and patients regarding the frequency and volume of heavy periods a smartphone app called Sisterhood (sisterhoodapp.com) was created to empower the patients to track their menstrual periods. Critical to improving awareness and educating the general public is collaboration. HFA and FWGBD created a brochure for providers highlighting the resources available and another brochure targeting the patients at risk for bleeding listing the typical bleeding signs and symptoms of a congenital bleeding disorder.
The NHF and the CDC collaborated on multiple materials focused on WWBD. The CDC has recently updated their materials and information on WWBD (cdc.gov) focusing on recently published research and the impact of a bleeding disorder on the lives of women with bleeding disorders. Betteryouknow.org is a website for undiagnosed women and men experiencing bleeding symptoms. The campaign was formed to create awareness and provide online resources to improve the time to diagnose a bleeding disorder. The materials are available from the CDC website and directly from betteryouknow.org.
The Canadian Hemophilia Society (hemophilia.ca) has long provided resources for WWBD and Code Rouge was a focused initiative to improve the time to diagnose a bleeding disorder for women with reproductive tract bleeding (heavy menstrual bleeding and perimenopausal bleeding).
To support their mission, they have meetings bringing together healthcare providers to educate, disseminate best practices, and debate controversial topics.
Focusing on the most common bleeding symptom in WWBD, Dr. Paula James (my personal clinical research hero) of Queens University created a website (letstalkperiod.ca) with an online version of bleeding score (ISTH Bleeding Assessment Tool) that allows at risk women to answer a brief bleeding inventory and determine whether they may be at risk for a bleeding disorder such as von Willebrand Disease. This sort of direct to patient initiative empowers women to advocate for themselves and arms them with objective bleeding information to approach their primary care provider or hematologist. Additionally, Dr. James’ initiative like the aforementioned organizations is deft at using social media to increase awareness.
List of Coagulation studies needed for WWBD
To appropriately evaluate the bleeding tendency of a woman or girl at risk for a bleeding disorder, the best first step is to objectively list the bleeding symptoms. One of the best methods to do this is to use the ISTH Bleeding Assessment Tool (ISTH BAT). This is available online via letstalkperiod.ca, academic website (bleedingscore.certe.nl), and the CDC.
A typical approach would be if there is an abnormal bleeding score (≥ 6 for females, ≥ 4 for males) a laboratory battery should be considered. This typically includes a CBC, PT and aPTT, Fibrinogen activity, and VWD profile of labs. The usefulness of the PFA-100 is widely debated and thus not routinely ordered. If this evaluation is negative, then it is reasonable to consider repeating the VWD profile particularly if the results are <100% and ordered with a platelet aggregation study (whole blood impedance or light transmission aggregometry.)
Complete blood count: Includes the hemoglobin and platelet count.
PT and aPTT: Prothrombin time and Partial thromboplastin time. This “bleeding time” can determine whether there is a significant reduction
of certain clotting factors. It is limited in that mild reductions may be missed. FXIII deficiency will not be screened for using PT and aPTT.
Fibrinogen: This is a clot-based assay that can
be used to screen for fibrinogen deficiency or dysfibrinogenemias. There is also a fibrinogen antigen that can be used if this activity assay is low.
Factor assays: Depending on whether there is a family history of a certain factor deficiency, individual factor levels may be sent. This includes FII, FV, FX, FXI, FVIII, FIX, FVII. FXIII is rarely sent due to the prevalence being less than 1 in 1 million.
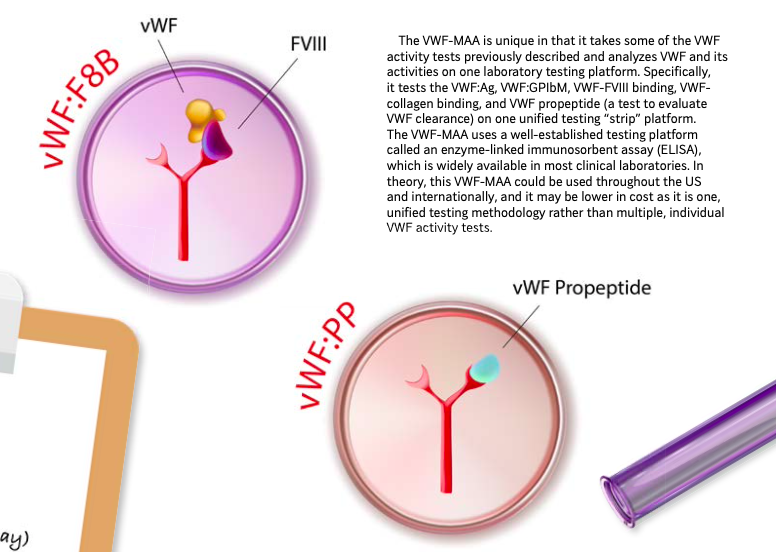
5. VWD profile: This typically includes the VWF antigen (VWF:Ag) a functional assay (VWF:RCo or VWF:GPIbm) and FVIII (factor 8 activity). Often times this assay may need to be repeated particularly if obtained
when severely anemic or during illness. A number of additional studies that can be sent depending on the initial results of the above. Certain labs will use the VWF:CB (collagen binding assay) to screen for type 2 VWD instead of using multimer distribution evaluation (how the VWF looks on a gel and whether all portions of it are present).
6. If the above is negative and there is concern for a qualitative platelet disorder it is reasonable to consider sending platelet studies (typically whole blood impedance or light transmission aggregometry). Basically, these tests evaluate how well your platelets work and react to certain reagents.
RESOURCES
As part of largely collaborative efforts a significant number of resources for both healthcare providers and patients have been created.
CDC.gov has a fact sheet about symptoms of bleeding in WWBD
(Betteryouknow.org is a collaboration between NHF and the CDC)
Postcard advertisements focused in improving awareness of WWBD
Menstrual chart and scoring system (Pictorial Bleeding Assessment Chart)
Teen booklet focused on discerning between normal and heavy menstrual bleeding
Doctor visit preparation list to improve communication between provider and patient
Healthcare diary list to focus the conversation on bleeding symptoms and signs
Lab test log to compile a list coagulation studies that may have been obtained from various healthcare systems
Testing booklet that explains the various coagulation studies important for making an appropriate diagnosis of a bleeding disorder
LetsTalkPeriod.ca has an electronic online version of the self-BAT, a self-administered version of the ISTH Bleeding Assessment Tool) assigning a score determining whether a woman or girl is at risk for a bleeding disorder such as von Willebrand Disease
NHF (National Hemophilia Foundation - Hemophilia.org) includes MASAC's (Medical and Scientific Advisory Council) guidelines (#251 and 245) focused on perinatal care and general recommendations for WWBD.
Victory for women (victoryforwomen.org) website focused on supporting WWBD and creating a community for conversations and general support.
HFA (Hemophilia Federation of America
- HemophiliaFed.org) offers the Women Bleed Too! Toolkit includes HFA/FWGBD brochures focused on bleeding symptoms to help identify women with possible bleeding disorder and educational patient directed materials. Sisterhood smartphone app which is an electronic version of the PBAC (Pictorial Bleeding Assessment Chart)
FWGBD (Foundation for Women & Girls with Blood Disorders - FWGBD.org) has made collaborative efforts with HFA above
Library of published papers focused on WWBD and compiled guidelines and an “ask the experts” option
List of clinics and level of resources focused on women and girls with bleeding and blood disorders
Ongoing Research projects in WWBD
There are a number of ongoing clinical initiatives addressing WWBD and I will highlight a few. ATHENA1 is an ATHN DREAM Award project led by Dr. Kristina Haley focusing on characterizing WWBD enrolled in the ATHNdataset. Recently, she described nearly 9,000 WWBD in the largest cohort to date. Of note, it highlighted our need for better focus on medical management of heavy menstrual bleeding.
The VWDMin (Von Willebrand Disease Minimize Menorrhagia) study (NCT02606045) is evaluating the usefulness of Tranexamic acid and a VWF concentrate in the reduction of heavy menstrual bleeding in adolescent and adult women with low VWF and VWD. It is ongoing and led by Dr. Margaret Ragni
from the University of Pittsburgh. The University of Miami Hemophilia Treatment Center has an investigator-initiated surveillance study for women with any bleeding disorder between the ages of 16 – 40. The participants will complete a questionnaire, undergo a physical therapy evaluation, and have on-site ultrasound imaging of their knees, elbows and ankles (the “index joints”) with enrollment occurring at the National LadyBugs Women’s Summit presented by the nSpiration
Foundation in collaboration with CHES (Comprehensive Health Education Services.)
Unmet Research Needs
As I see it, there are a number of unmet needs in WWBD. I will highlight a few that I feel need to be addressed soon, and certainly there are more to address.
1. We do not understand how much a congenital bleeding disorder, such as VWD or hemophilia carriage, contribute to the severity or irregularity of heavy menstrual bleeding or any reproductive tract pathology. To that end we need to focus on the pathophysiology of uterine bleeding (period bleeding and menopausal bleeding). We do not know whether a bleeding disorder leads to anatomic defects or alteration of the blood vessel formation leading to irregular and prolonged periods.
2. We do not fully understand why there is a discrepancy in bleeding symptoms and severity of clotting factor deficiency. This is noted particularly in men with mild VWD and in rare bleeding disorders, but it seems to be more pronounced in WWBD. For example, we have not been able to determine why a woman with a FVII level of 35% may bleed more than one with a level of 5%, and why women with hemophilia and mild factor deficiency have similar bleeding tendencies as those with normal levels. Even more of a challenge is in those with low VWF and mild VWD. The range of bleeding is quite large and likely due to the multiple genetic causes of reduction of VWF in humans.
3. We are not able to accurately predict bleeding with day to day events and with procedures, particularly in those with very mild factor deficiencies. Larger prospective studies will be needed to address this issue.
4. The pathognomonic bleeding symptom of hemarthrosis in hemophilia is poorly described in hemophilia carriers and those with mild, moderate and severe deficiency. Better documentation and evaluation of treatment outcomes will ensure better communication between providers and patients.
5. We have not been able to prospectively evaluate the role of hemostatic agents and hormonal agents (birth control pills, IUDs, and progestin only pills) in the medical management of heavy menstrual bleeding. We have not been able to effectively conduct clinical trials in this group due to the inherent challenges of infusions of CFCs (clotting factor concentrates) at the onset of the period. The majority of persons with VWD do not know how to infuse (due to infrequent IV infusions in general), certainly a much lower rate than those with hemophilia. Currently the VWDMin study (NCT02606045) is evaluating the usefulness of Tranexamic acid and a VWF concentrate in the reduction of heavy menstrual bleeding in adolescent and adult women with low VWF and VWD. To date, no prospective study of the role of FVIII or FIX concentrate has been executed in hemophilia carriers, again due to the complexity of infusions on the first day of the period and lack of large enough participation.
6. We need further investigation of the role of imaging, such as musculoskeletal ultrasound and MRI in surveillance of possible joint damage/bleeding particularly in the women and girls with mild and moderate clotting factor deficiency – more specifically in hemophilia and VWD.
7. We need a more inclusive registry or surveillance system. Potentially we could leverage the resources of NHF and ATHN for better longitudinal evaluation and there will be an international effort with ISTH (International Society of Thrombosis and Hemostasis) soon to collect data on hemophilia carriers and VWD patients. Women and girls with bleeding disorders are currently part of the CDC Community Counts initiative (part of the ATHN data collection) and are included in the general authorization into the ATHNdataset. I believe a focused registry is needed to be able to answer some of the questions posed and to encourage larger scale participation.
With continued ongoing collaborative efforts from the patient advocacy groups, medical research societies, government, and pharmaceutical industry we can address the unique medical and research needs of WWBD. In my relatively short career, I have seen a concerted effort and only see continued dedication from the next generation of young investigators.
Dr. Sidonio is an Assistant Professor of Pediatrics, Emory University School of Medicine, Clinical Director of the CHOA Hemophilia Treatment Center, and the Associate Director of Hemostasis and Thrombosis, Department of Pediatrics, Children’s Healthcare of Atlanta. The focus of his clinical research career has been on understanding the prevalence of congenital bleeding disorders such as low VWF, qualitative platelet disorders or hemophilia carriage in adolescent girls and women with heavy menstrual bleeding and the diagnosis and management of women and girls with bleeding disorders. Dr. Sidonio has multiple national leadership and/or working group roles in every major hemostasis organization. Notably, Dr. Sidonio is the national PI for a recently awarded grant called ATHN 9 (severe VWD), Mexico Inhibitor Study (natural history of inhibitor development in Mexico) and Emicizumab PUP and Emicizumab ITI study.